|
By
Dawn Brazell
Public Relations
Jim Hoshour teaches
business classes as Sumter High School, captures film footage as the
video coordinator for the football team, coaches the prestigious
American Legion Baseball P-15 team and loves to spend time with his 11
grandchildren.
 Jim Hoshour, right, with son, Chad
Hoshour and grandson, Jackson. With 11 grandchildren, Hoshour said he
wanted to be proactive in seeking the best treatment for his bladder
cancer that would keep him active. Jim Hoshour, right, with son, Chad
Hoshour and grandson, Jackson. With 11 grandchildren, Hoshour said he
wanted to be proactive in seeking the best treatment for his bladder
cancer that would keep him active.
When he found out he had
muscle-invasive bladder cancer, he didn't just want to know if he could
fight it, he wanted to know how to fight it and still have an active
and good quality of life.
Harry Clarke, M.D., Ph.D.,
associate dean for graduate medical education and urologist, knew he
had the perfect candidate for what would be MUSC's first robotic
cystoprostatectomy, or the removal of the bladder and prostate that
included taking a part of Hoshour's bowel to reconstruct a new bladder
called a neobladder. If all went well, the neobladder would mean
Hoshour would not have to wear a bag or use a catheter.
"He has done really well
and has been able to void on his own. It's the best of all worlds as
far as his outcome. I counsel patients who 8 out of 10 will be able to
void on their own, but 2 out of 10 will have to use a catheter."
Hoshour thought those were
good averages, and said he didn't mind being MUSC's first patient to
have this procedure done using the robotic da Vinci Surgical System. A
photographer and videographer, he's comfortable with high-tech
equipment and had confidence in Clarke's decision, he said.
The da Vinci Surgical
System, developed by the U.S. Department of Defense, was introduced to
MUSC in May 2008 by Andre Hebra, M.D., director of the Division of
Pediatric Surgery. Since then, the use of the system has spread to a
variety of specialties, including urology. The challenge now is
competing with other specialties to find time on the machine, Clarke
said.
He likes the versatility
of the machine, especially with the new devices that have been
developed to expand its uses. "I think in the next 10 years or so,
we'll be doing more and more things robotically. We've already seen
that evolution with laparoscopy. We're doing more things
laparoscopically then we ever thought we'd be able to do. Certainly,
we'll do more things robotically."
The robotic system
features four interactive robotic arms equipped with instruments
designed with seven degrees of motion, which allows various surgical
functions such as clamping, suturing and tissue manipulation. A camera
and light is mounted on one arm providing high-definition, 3D videos
that are displayed throughout the operating room. Surgeons sit at a
console where they can manipulate all four robotic arms via hand and
foot controls.
"We've started in the past
couple of years doing more and more cases with the da Vinci robot. As
we're getting more and more comfortable, we're able to push the
envelope a little bit," he said, explaining how it allows them to take
on more complicated cases. "This is the first one in South Carolina
where we've done a neobladder."
Robotic surgery has
received some negative criticism lately by health professionals
concerned that it's being over-marketed. Some research suggests the
robotic procedure reduces hospital stays and blood loss, compared with
regular surgery, but studies have also shown that robotic surgery
offered no added benefit or worse results.
 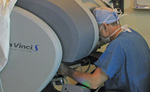 Dr.
Harry Clarke uses the da Vinci surgical console, which has hand and
foot pedals to operate four mechanical arms. Right, one of the video
monitors during a recent procedure with a video link at http://bit.ly/MUSCdaVinciSurgicalSystem.
Hoshour's procedure was the first continent orthotopic neobladder done
robotically at MUSC. Dr.
Harry Clarke uses the da Vinci surgical console, which has hand and
foot pedals to operate four mechanical arms. Right, one of the video
monitors during a recent procedure with a video link at http://bit.ly/MUSCdaVinciSurgicalSystem.
Hoshour's procedure was the first continent orthotopic neobladder done
robotically at MUSC.
As with any medical
procedure, each case needs to be decided on its own merits, said
Clarke. Robotic surgery may not be the best choice of approach for some
patients given their medical history and condition. Clarke's advice to
patients is to not assume the newest and latest equipment and/or
procedure is the best for them, but to ask questions.
For certain procedures,
Clarke said he has found there is less fluid loss when done
robotically, and he has found recovery time tends to be quicker. The
magnification the da Vinci and the manipulative arms allow surgeons to
get around difficult areas easier, he said.
"In certain situations the
anatomy is such that the robot is very helpful. The magnification,
dissecting the nerves – all those things are better done. Certainly
when there's a deep pelvis and to tie off the vessels, it makes it
easier to do."
 Dr. Harry Clarke Dr. Harry Clarke
Clarke, who's pleased to
see how well Hoshour, 65, is doing, said he was an ideal candidate
because he was active and healthy. Clarke took a 45 cm segment of small
intestine, the ileum, and constructed a pouch that retains its blood
supply from the bowel, and when brought down and attached to the
urethra, acts as a bladder.
Hoshour, who found his
cancer in January 2010 after going for a run and coming home to
discover a massive amount of blood in his urine, said he wanted to try
for the option that would require the least change in lifestyle. After
getting his diagnosis, he received immunotherapy and then had surgery
in April this year when he received the neobladder.
Glad he didn't wait to seek treatment, Hoshour, 65, said he's back to
his loves of sports, coaching and photography.
 Hoshour coaching the P15 American
Legion team this month. Hoshour coaching the P15 American
Legion team this month.
"There's no use in sitting
around. Life's too short," Hoshour said. "I have 11 grandkids to keep
up with."
|


